Hypothyroidism is one of the causes of hyponatremia, thus thyroid-stimulating hormone determination is mandatory during the evaluation of patients with reduced serum sodium levels.
Can hyperthyroidism cause hyponatremia?
Myxedema coma, characterized by chronic extreme thyroid-stimulating hormone (TSH) elevations, has repeatedly been linked to the development of hyponatremia [6,7,8], among many other complications.
Can thyroid cause electrolyte imbalance?
Our study demonstrated that hypothyroid patients show serum electrolyte disturbances such as low sodium, low potassium, low calcium levels and high magnesium and phosphorus levels.
Why does hypothyroidism cause low sodium?
The main mechanism for the development of hyponatremia in patients with chronic hypothyroidism is the decreased capacity of free water excretion due to elevated antidiuretic hormone levels, which are mainly attributed to the hypothyroidism-induced decrease in cardiac output.
What are the warning signs of hyponatremia?
Hyponatremia signs and symptoms may include:
- Nausea and vomiting.
- Headache.
- Confusion.
- Loss of energy, drowsiness and fatigue.
- Restlessness and irritability.
- Muscle weakness, spasms or cramps.
- Seizures.
- Coma.
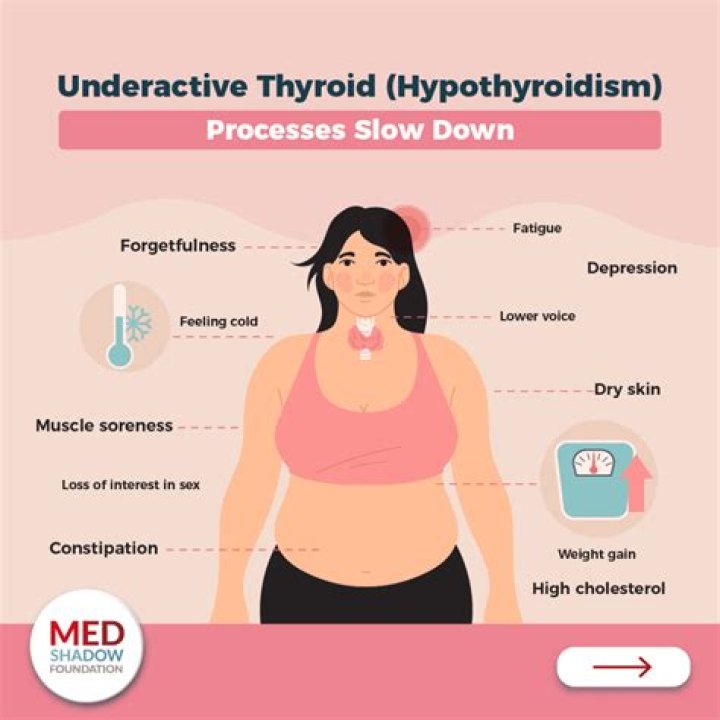
Can hypothyroidism cause electrolyte imbalance?
Hypothyroidism is one of the most prevalent endocrine diseases. It can lead to a variety of clinical situations, including congestive heart failure, electrolyte disturbances and coma. Hyponatremia is the most common electrolyte abnormality encountered in clinical practice (Kargili A et al, 2010).
How does hypothyroidism cause hypoglycemia?
Hypothyroidism is linked with various hormonal biochemical and nervous system abnormalities, which may contribute to hypoglycemia. The condition is linked with low growth hormone and cortisol responses to insulin induced hypoglycemia, and this prevents adequate counter regulatory protection.
Why does SIADH cause hyponatremia?
The syndrome of inappropriate secretion of antidiuretic hormone (SIADH) is a disorder of impaired water excretion caused by the inability to suppress the secretion of antidiuretic hormone (ADH) [1]. If water intake exceeds the reduced urine output, the ensuing water retention leads to the development of hyponatremia.
What is the difference between hyponatremia and SIADH?
In SIADH, hyponatremia is caused by water retention due to inappropriate secretion of antidiuretic hormone (ADH) (10-15). But in CSWS, hyponatremia is associated with high urine output, high urine sodium concentration, and plasma volume depletion (16).
What is the prevalence of hyponatremia in the United States?
United States. The incidence of hyponatremia depends largely on the patient population and the criteria used to establish the diagnosis. Among hospitalized patients, 15-20% have a serum sodium level of < 135 mEq/L, while only 1-4% have a serum sodium level of less than 130 mEq/L. The prevalence of hyponatremia is lower in the ambulatory setting.
What are the possible complications of rapid correction of hyponatremia?
Correction of serum sodium that is too rapid can precipitate severe neurologic complications. Most individuals who present for diagnosis, versus individuals who develop it while in an inpatient setting, have had hyponatremia for some time, so the condition is chronic, and correction should proceed accordingly.
How common is hyponatraemia in patients with high TSH levels?
Hyponatraemia was present in 14% of patients with high TSH and was significantly more common than in the group with normal TSH levels of which 9% had hyponatraemia (p <0.01). Hypokalaemia was more common in the group with elevated TSH than in those with normal TSH (14 versus 11%, p = 0.016).
What tests are used in the workup of hyponatremia?
Ancillary tests. After correction of hyponatremia, the hypouricemia corrects in SIADH but remains with a salt-wasting process. Thyroid-stimulating hormone (TSH) and serum cortisol levels should be measured if hypothyroidism or hypoadrenalism is suspected.