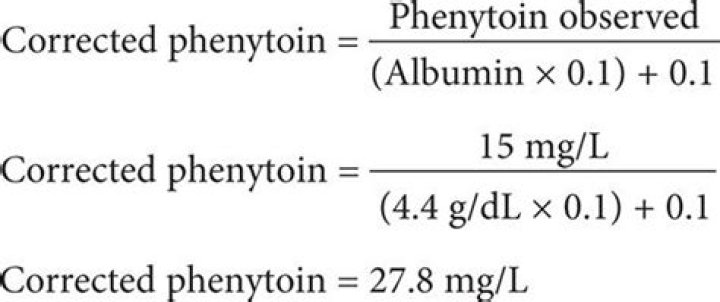
Corrects serum phenytoin level for renal failure and/or hypoalbuminemia. Use in patients with albumin ≤3.2 g/dL (32 g/L). The “Sheiner-Tozer Equation” is the official name of this correction.
How does albumin affect phenytoin levels?
Serum albumin concentrations < 3.5 g/dL have previously been shown to affect phenytoin binding ratios and to contribute to phenytoin intoxication. Decreased protein binding leads to an increase in the free fraction of the drug.
Does phenytoin bind to albumin?
Phenytoin is mainly bound to albumin, the percentage of bound drug being constant over a wide range of total drug concentrations.
Can phenytoin cause hypoalbuminemia?
Phenytoin has a high protein binding (90%), so hypoalbuminemia condition will affect the free drug amount in the body, while it is known that only drug that unbound by protein (free drug) who can pass through the membrane and reach its target.
Why do we correct phenytoin?
Total serum phenytoin levels reflect both bound and unbound drug. However, as protein-bound phenytoin cannot cross the blood-brain barrier, only free phenytoin is active. In healthy adults, approximately 90% of phenytoin is bound to albumin. Thus, phenytoin levels must be corrected according to albumin levels.
What is corrected phenytoin level?
Corrected phenytoin levels were calculated using the Sheiner-Tozer equation. Corrected phenytoin levels = Measured total phenytoin(micromol/l) [(albumin g/1 x 0.9)+ 0.1] 40. Results: At Visit 1, mean serum albumin levels were 44.1 +/- 1.1 micromol/l and mean serum phenytoin levels were 33.9 +/- 2.8 g/l.
How do you calculate corrected albumin?
Formula Used: Corrected Ca = [0.8 x (normal albumin – patient’s albumin)] + serum Ca level.
What interacts with phenytoin?
Most frequently checked interactions
- Acetylsalicylic Acid (aspirin)
- Advair Diskus (fluticasone / salmeterol)
- Aspirin Low Strength (aspirin)
- Combivent (albuterol / ipratropium)
- Coumadin (warfarin)
- Keppra (levetiracetam)
- Lasix (furosemide)
- Lipitor (atorvastatin)
What causes phenytoin toxicity?
Phenytoin toxicity can occur from an increase in the daily dose of phenytoin, changes in the formulations or brands as well as changes in the frequency of administration. It can also occur when patients are started on new medications that interact with the metabolism or binding capacity of phenytoin to plasma proteins.
How is phenytoin eliminated?
Much of the drug is excreted in the bile as an inactive metabolite, which is then reabsorbed from the intestinal tract and ultimately excreted in the urine. Less than 5% of phenytoin is excreted unchanged in the urine.
When Should albumin be corrected?
Therefore, to correct for an albumin level of less than 4 g/dL, one should add 0.8 to the measured value of calcium for each 1-g/dL decrease in albumin. Without this correction, an abnormally high serum calcium level may appear to be normal.
What happens when Dilantin level is too high?
Drowsiness, especially excessive drowsiness, is also a signal that Dilantin levels are too high. Dilantin toxicity can lead to involuntary jerking movements. These involuntary movements can involve the body, the face or the arms and legs.
How often to check phenytoin level?
With recommended dosage, a period of seven to ten days may be required to achieve steady-state blood levels with phenytoin and changes in dosage (increase or decrease) should not be carried out at intervals shorter than seven to ten days.
When to check phenytoin levels?
It may be ordered every few days when a person first begins taking phenytoin to help adjust the dose to the desired blood level. The test is then ordered at regular intervals and as needed to monitor blood concentrations.
How to treat elevated Dilantin levels?
Diet & exercise: Moderate exercise (about 30 minutes 5 times a week) reduces LDL cholesterol and raises HDL cholesterol. Smoking can lower HDL levels, so stop smoking if you do. Eat lots of fruits, vegetables, whole grains and lean sources of protein. Include monounsaturated fats in your diet – …Read more.